
I went for the Autism cure, but all I got was a ‘Don’t Tylenol’ T-shirt !
HHS Secretary Kennedy: 40 life-death actions you can't put off any longer !
Please share this so that it might eventually reach him, and along the way, wake many people up, saving many lives.
From VaxiNazi to Anti-Haxxer in 30 seconds:
Help wanted: I need a volunteer to make this video with the raw files.
We need this irrefutable, unassailable, indisputable, incontrovertible, unquestionable, conclusive, definitive, certain, unarguable, undebatable, compelling, convincing, amazing tool for viral campaigns and to add in QR cards posted everywhere!
1. This image SAVES LIVES:
Skip to the end for the full explanation.
2. Shocking 20 sec video:
Except for Graphene, there is no other explanation for a para-magnetic element that reverses polarity and has so much magnetic power, even though the injection is half a cubic millimeter (0.5 mm3) and powers a Bluetooth micro-router.
Share or download here.
3. Heartbreaking 20 sec video:
2016. UK. Luke Maguire and Louise McKever, after a bad reaction to the first dose of Glaxo’s Bexsero Meningitis B vaccine (given to babies at 2, 4 and 12 months), and after being threatened of removing their child if they didn’t comply with the second dose, they witnessed that it caused Bobby to have daily fits. To prevent other parents, they shared this video on Facebook. You may download the video here: https://odysee.com/@nazar:d/seizures12:9
We are expecting an answer from the HHS:
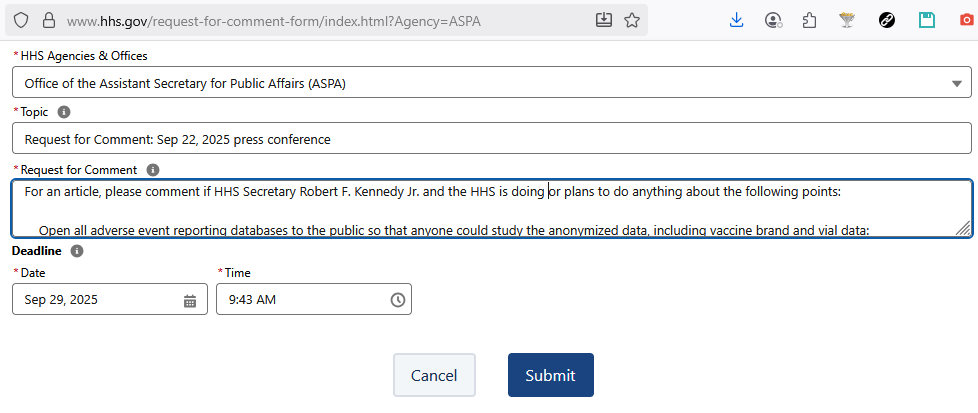
https://www.hhs.gov/request-for-comment-form/index.html?Agency=ASPA
This article triggered the censorship AI
Not being enough that my X account was completely shadow banned (no one gets my posts, not even my followers), it was blocked after I posted a link to this article. After unblocking it through an “prove that you are human” puzzle, I got this message:
Live-stream announcement Sep 22, 2025
Trump recommended
Avoid Tylenol during pregnancy and giving it to the baby
Note: including through breast-milk.
Note: Tylenol is acetaminophen, also known as paracetamol, is a non-opioid analgesic and antipyretic agent used to treat fever and mild to moderate pain. It is available over-the-counter under various brand names, including Tylenol and Panadol. Also, Nonsteroidal anti-inflammatory medications (NSAIDS), such as ibuprofen (Advil) and aspirin, can cause reduced blood flow, heart problems, and kidney problems in the unborn child.Avoid vaccines with aluminum and mercury (neurotoxic) and that they are trying to take them out of the injections.
Avoid Hepatitis B vaccine until 12 years-old because it’s a sexually transmitted infection
Note: why are they on the Schedule if newborns are not sexually active! If some want to follow God’s good advice to remain virgins until a lifelong faithful happy marriage, why should they be vaccinated against Sexually Transmitted Diseases, they’ll NEVER get, like Hep B and HPV?
Avoid the MMR vaccine and take them separately, 1 for measles, 1 for mumps and another for rubella, but in different doctor visits.
At least, spread vaccines along years, never all in one visit, considering it’s 80 immunizations
The REAL meaning of a recommendation to space vaccines
Read between the lines: it means that “the poison is in the dose”.
By spreading out or spacing them, you reduce the dose of poison and its effects, since the body has more time and resources to fight the deadly invasion.
It’s just like a “loving” spouse giving tiny doses of arsenic with the “lovingly” prepared food: if the dose is too high, it will raise and investigation, but if it is spread out, then the victim just fell sicker and sicker and the doctors are clueless. Masonic Big Pharma and HHS are the murdering spouse of the people with the “lovingly” prepared “vaccines that save lives”.
The criminal intent was proven by howbad.info proving that the more lethal vials were pre-labelled as highly toxic with special standard codes: check your batch code!
Sink this in: would you receive an injection from a vial with a skull&bones, biohazard or radioactive label? Well, 5% of the population did and most are dead or dying by now.
Imagine a Biohazard Level 4 (BSL-4) label: biological substances that pose an incurable life-threat to living organisms, especially humans (suitable for areas with biological experiments or quarantine zones like the Wuhan lab creating and releasing COVID):

Or radioactive, since radioactive elements were found in the vials and Technetium in the swabs:

During Q&A, Trump refused to answer the question of a CNN reporter: “Not CNN, you are fake news” =)
Trump recalled the case of a mother losing his wonderful boy to autism the day after a vaccine followed by a very high fever (typical vax autism regression).
Trump said
Autism went from 1:10,000 to 1:10 in California (1000x!).
Cuba has less autism because they take less Tylenol (true, they have less than half the USA rate).
The Amish have no autism (true, it means that the agri-chemical, processed food and pharmaceutical industries are the obvious suspects!).
He believes in vaccines.
He’s still proud of Operation Warp Speed COVID vaccines.
Open letter to Robert Kennedy Jr.
Thank God for all the good things you did, but it’s clearly not enough. At bottom, the ultimate proof that hackcines cause autism.
You were sworn in on February 13, 2025, 7 months ago.
We are closely watching you. You’ve enabled many positive things:
30 Apr 2025. You announced (of all media, why did you chose the masonic Washington Post?) a shift in policy that would require all new vaccines to undergo safety testing in placebo-controlled trials: why not requiring this also for all the old ones, since none presented double-blind, placebo-controlled studies?
Note for readers: it is a clinical trial where neither the participants nor the researchers know who is receiving the active treatment and who is receiving a placebo. This “double-blinding” minimizes bias from both participant expectations (the placebo effect) and researcher bias, making it the “gold standard” for assessing a treatment’s effectiveness by ensuring that the observed outcomes are due to the treatment itself, not other factors.
1 May 2025. Wonderful HHS gender dysphoria report, Treatment for Pediatric Gender Dysphoria: Review of Evidence and Best Practices, possibly prevented and will prevent the brutal mutilation (“transitioning”) of thousands of minors. The proof of your good job was the dominant media criticism, including the American Academy of Pediatrics, for misrepresenting the “medical consensus”, based on ideology, threats and bribes, not evidence.
9 Jun 2025. Expelling the whole board of 17 VaxiNazi “experts” in the CDC Advisory Committee on Immunization Practices (ACIP), the CDC’s key vaccine policy and recommendation panel, citing conflicts of interest and a need to restore public trust in vaccine science, which deserves a standing ovation, except for naming CIA-asset Robert Malone.
24 Jun 2025. The new ACIP panel voted against neurotoxic mercury (thimerosal) in any vaccine. From 1999 to 2001, it was removed from all vaccines except influenza, after a US Public Health Service and the American Academy of Pediatrics had recommended full removal. Keeping mercury for 26 years proves how corrupt the previous panels were. Also, that mercury was not the main cause of autism. Many countries still use thimerosal as preservative in vaccines and other medications (nasal drops!).
18 Jul 2025. HHS formally rejects WHO’s 2024 International Health Regulations amendments, because they expand WHO authority over U.S. public health policy. Yet, the USA didn’t leave that treaty, yet, as well as the WHO and PAHO treaties, which means that when Trump is gone, they could easily be resumed.
23 Jul 2025: One month too late, HHS adopted the recommendation from the new ACIP panel to remove mercury from the influenza vaccine.
5 Aug 2025: “HHS Winds Down mRNA Vaccine Development Under BARDA” 22 projects involving 500 million dollars.
Termination of contracts with Emory University and Tiba Biotech.
De-scoping of mRNA-related work in existing contracts with Luminary Labs, ModeX, and Seqirus.
Rejection or cancellation of multiple pre-award solicitations, including proposals from Pfizer, Sanofi Pasteur, CSL Seqirus, Gritstone, and others, as part of BARDA’s Rapid Response Partnership Vehicle (RRPV) and VITAL Hub.
Restructuring of collaborations with DoD-JPEO, affecting nucleic acid-based vaccine projects with AAHI, AstraZeneca, HDT Bio, and Moderna/UTMB.
While some final-stage contracts (e.g., Arcturus and Amplitude) will be allowed to run their course to preserve prior taxpayer investment, no new mRNA-based projects to be initiated.
HHS instructed its partner, Global Health Investment Corporation (GHIC), which manages BARDA Ventures, to cease all mRNA-based equity investments.
27 Aug 2025. You got VaxiNazi, Susan Monarez removed: the CDC director, who had endorsed the updated COVID poison (“vaccine”) for 6 months babies, protected the Big Pharma corruption, and endorsed the COVID response narrative.
27 Aug 2025. 195 days too late since you assumed (end of Federal COVID emergency was 11 May 2023), the day after my article on Public Health Emergency Over Infant Deaths due to COVID haccines, FDA rescinded the Emergency Use Authorization for COVID vaccines (yet, leaving the biobombing authorization for the elderly and comorbid).
18 Sep 2025. Sanctions announced against organ transplant agency in Florida: it might be a start to stop widespread organ harvesting.
19 Sep 2025. ACIP says that COVID-19 injections are an individual decision, not a universal recommendation.
22 Sep 2025. NIH launches $ 50 million dollars for Autism research in 13 projects: why is it that those organizations were compromised with the COVID response anti-scientific ideologies, and none is a vaccine truther? Why would this top priority be only 0.004% of your 7 month spending ($176.6 billion/month)?
22 Sep 2025. About autism, you said “this administration is determined to look at everything—the environment, vaccines, food supply, parenting methods, water, and air—as potential contributors to the autism epidemic. Everything is on the table. We are committed to an honest and thorough investigation, free from political influence and industry pressure.” Though,
Parenting methods have nothing to do with autism! Stop blaming the parents in this endless blame-game, always beating around the bushes, but never reaching the center: the massive corruption in the Government-Pharma-Healthcare Industrial Complex!
The big fat pink elephant in the room? what about the side effects of agrichemicals (“fertilizers”, pesticides, fungicides, herbicides) and chemtrails, not only on autism but on all the chronic diseases? Is it because in the confirmation hearings you said you would not mess with the corrupt Environmental Protection Agency (EPA) and the U.S. Department of Agriculture (USDA)? Has anyone tied your hands in this? Why don’t you denounce them?
Plan to cut 10,000 jobs from the HHS, while consolidating regional offices.
Plan to remove aluminum (neurotoxic) from all vaccines (substitute worse?).
We know that:
You know how lethal and maiming those weaponized injections are: we’ve read your books.
You are surrounded by wolves in sheep’s clothing, like mason Dr. Oz (admin of CMS): his supplement company, iHerb, sells folinic acid
You are playing 5D chess on a tight rope.
You are not allowed to do anything controversial without Trump’ support and that, because he still wants his re-election, meaning, he still cares for Big Pharma funding, Vax-votes and impeachements based on manufactured cases.
If Trump fires you, or you are impeached, your political career is practically over. Who else is going to Make America Healthy Again?
Notwithstanding, since you assumed:
Children were given 3 million doses of the autism-inducing MMR haccine, especially after your misinformation on 6 Apr 2025: “The most effective way to prevent the spread of measles is the MMR vaccine.” (I’ll refute that statement with science ASAP).
9 million children got injected the COVID bioweapon.
75 million minors were injected the “vaccine schedule” poison … on your watch!
Every day that goes by, more children get handicapped, maimed, infertilized or dead by the haccines: all injections, including those in the vaccine schedule have been weaponized to reduce the population by 95%, leaving only 5%). Time means lives !
In these 7 months, HHS spent $1.295 trillion of tax-paid dollars!
Yet, on Sep 22, 2025, all you did was point to Tylenol as the main cause for autism and that the only action to improve symptoms of autism, it is to take leucovorin (folinic acid, vitamin B9) and wait for more studies!
Yet, there are so many things you could have done and should still do:
Integrate and open all databases (20+) which enable the study of adverse effects, so that anyone could study the anonymized data, including vaccine brand and vial data:
Vaccine Adverse Event Reporting System (VAERS)
Vaccine Safety Datalink (VSD)
Defense Medical Surveillance System (DMSS) and its Defense Medical Epidemiology Database (DMED)
Vaccine Adverse Event Clinical System (VAECS)
HHS prescription data
Secret databases run by the Bio-defense Industrial Complex, at least those about the vaccines rolled out in the market or deployed on the military human guinea-pigs, in their war-on-terror-caused-by-bugs.
Drug Enforcement Administration (DEA): pharmacies must report their controlled substance (Schedules II-V) inventory and sales, and under court order, individual prescription records.
Centers for Medicare & Medicaid Services (CMS): as part of the Consolidated Appropriations Act, 2021, health insurance companies and employer-based health plans must submit prescription drug data to CMS for the Prescription Drug Data Collection (RxDC) report.
Civil Aerospace Medical Institute (CAMI) Incapacitation Data Registry (IDR), suspiciously shut down in 2021
Pilot Records Database (PRD)
Pharmacy Benefit Managers (PBMs): third-party administrators of prescription drug programs for health insurance companies and large employers, with extensive access to prescription data to manage benefits and process claims. Largest PBMs: CVS Health (Caremark), Cigna (Express Scripts), UnitedHealth Group (OptumRx).
Prescription Drug Monitoring Programs (PDMPs): state-level electronic databases that track prescriptions for controlled substances. Used by healthcare providers and authorities to identify patterns of misuse, prevent overdose, and inform clinical decisions.
Ambulatory Care Drug Database System (CDC): data on drug use based on physician entries from the National Ambulatory Medical Care Survey (NAMCS).
ClinCalc DrugStats Database: prescription drug use in the U.S. based on data from the Medical Expenditure Panel Survey (MEPS). It ranks drugs by total prescriptions and has other statistics.
nSIDES: This database, compiled from DailyMed data (National Library of Medicine), focuses on drug side effects and interactions. It processes drug labels to extract information on drug-adverse event pairs.
Drug Information Database (National Medical Association): Powered by phactMI, this resource provides a comprehensive, evidence-based database of drug information for healthcare professionals.
Databases from vaccine developers and manufacturers, currently siloed and confidential, in spite that they were funded by the taxpayers, through grants and billion-dollars government vaccine direct contracts and purchases.
Data analytics firms: Companies like Symphony Health and ValueCentric receive prescription data from pharmacies to generate market research and pharmacy risk scores.
Electronic prescription services: Companies like Surescripts facilitate the secure electronic exchange of prescriptions and other health information between physicians, pharmacies, and PBMs.
Vaccine exempted: they are ideal for studies comparing vaxxed with unvaxxed.
Mandate vaccine adverse event reporting, which currently is about 1% of total cases because it is a voluntary system.
Mandate long term follow up of all medical products, including multivariate analysis of all-cause mortality.
The causation (or lack of it) between adverse side effects and the medical product, should be established by lab analysis, autopsies and independent studies, not Big Pharma or their mercenaries at the HHS!
Establish objective statistical safety signals, which should automatically trigger a fast response.
Guarantee database integrity with open logs, and severe punishment (fines and imprisonment) to those manipulating data, as previously detected: they are messing with public health policy, lives are at stake for wrong or partial information.
Create a daily live-streamed press conference, where peer reviewed studies are presented, one by one, and the vaccine injured tell their stories, one by one.
Show magnetism after vaccination live. Study why the unvaxxed have becomed magnetized, too (hint: other injections like dental anesthesia and IV). Study and warn about the risk of MRI scanning or magneto-therapy, a if the animal or person has reduced Graphene Oxide inside the body.
Showcase the science debunking the COVID response narrative: haccines, lockdowns, masking, social distancing.
Have the COVID haccines analyzed, by several labs and research centers, for what has already been found: plasmid DNA, Graphene Oxide, lanthanides, radioactive elements, micro-routers, etc. Use different labs to corroborate the results. Livestream the whole process with chain of custody.
With blood analysis show how the haccinated are still producing vax spike protein, which is different from the COVID one, as already proven.
Ban PCR as a diagnostic test to determine spreading potential. Publicly expose the PCR-fraud to prevent future PLANdemics.
Publish protocols to treat the vaccine injured and other diseases (like the FLCCC/AMA ones).
Remove liability protection to all Pharmaceutical companies, especially for all those products approved without proper independent conflict-free studies.
Establish that it’s Big Pharma, never the injured, who have to prove that there’s no link between the injection and the injury.
Grant generous compensations to the vaccine injured, paid by the vaccine manufacturers and entities that pushed them, including hospitals and corporations.
Create a research fund, where organizations representing the vax injured define grants: Childrens’ Health Defense, ICAN (Informed Consent Action Network), National Vaccine Information Center (NVIC), etc. Favor studies comparing the injected with the unhaxxed.
Exclude grants to any organization involved in the anti-scientific support of the COVID response narrative.
Establish that all studies receiving HHS funding must comply with open science, including publication of raw data. To reduce the pandemic of scientific fraud, non-replicable studies must return the funding with interest and fines.
Establish that any patent deriving from HHS funding is for the public domain within the USA, while patent income from abroad goes to the adverse events compensation program (not the HHS to reduce conflicts of interest in FDA approvals).
Publicly shame and prosecute Dr. Fauci and his gang of criminals (Biden’s Presidential pardon is void)
Ban mRNA and DNA haccine tech. Replace vaccines with widespread availability of cheap monoclonal antibodies or immunoglobulins.
Denounce the PREP act. Take all the possible steps to disarm it. It’s the fuse for the next PLANdemic, when you will not be in charge.
Enable ivermectin, HCQ, nitazoxanide, fenbendazole, mebendazole, Chlorine dioxide, as over-the-counter drugs (no need of prescription).
Fully enable alternative schools of medicine (integrative, holistic, Hildegardian, Germanic, Chinese, Indian, African, acupuncture, etc.), enabling medical insurance to cover them at the will of the patient.
Revert the definition of death to past standards, since the current definition is resulting in organ harvesting from live patients declared brain-dead.
Enforce real informed consent for every single medication and treatments including risks, numbers and percentages for each adverse event. Why not mandating signed informed consent e-forms, after the prescribing doctor reads and explains to the patient, all the adverse events in the package leaflet, with mandated follow up of those symptoms and VAERS updating?
Publish the study and the official transcription of the conspiracy vax meeting about Hep B vaccine, that you denounced. If all erased, why not denouncing the vanishing and redoing exactly that same study and a public inquiry or subpoena of those in that meeting?
Make the CDC publish the study whistle-blowed by Dr. Thompson (repeated by Dr Brian Hooker). Immediately expel from the HHS, those 4 scientists involved in scientific fraud, costing the lives of so many children and retract their paper.
Repeat the study from HowBad.info proving that the bad batches were pre-labelled as toxic, thus proving criminal intent.
On March 10, 2025, you directed the FDA to explore eliminating the "self-affirmed" Generally Recognized as Safe (GRAS) pathway for food ingredients, a loophole that let companies add new chemicals and ingredients with potentially unknown safety data, instead of publicly notifying the FDA of new ingredients and supporting safety data before market entry: why is there no resolution and why did you leave out medicines?
Aren't approval studies directly designed, paid and processed by the manufacturer a kind of self-affirmation with conflict of interest? Wouldn’t it be better that Pharmaceutical companies contribute to a research fund run by Government, leaving all of those roles to the FDA, so it could guide multiple studies by multiple institutions and non profits without conflict of interest?
Review the safety of aspartame and ban it. Also for statins, drugs similar to Vioxx, psychiatric drugs, oncology drugs and treatments, etc.
Is America going mad? 24,9%, 1 in 4 adults are taking psychiatric drugs, which were never recommended for long-use !!! Women twice as men, possibly because they are hidden that hormonal contraception may cause depression. Whites more than any other race. Healthy children are being hijacked by Big-Pharma-mercenary psychiatrists in a growing trend, especially involving Selective Serotonin Reuptake Inhibitors (SSRI), like the case of Danielle Gansky. For example, it’s proven by many studies that vaxxed children have 4x more attention deficit hyperactivity disorder (ADHD) than the unvaxxed, yet instead of curing the vaccine side effect, or preventing their younger brothers getting vax-injured, they are forced into lifelong drug dependence. COVID vax brain injury is treated with psycho-drugs instead of the IMA post-vac protocol.
The long-standing “chemical imbalance” theory of depression is wrong:High-quality meta-analyses of studies, involving tens of thousands of participants, have found no significant or consistent difference in serotonin concentrations (or its primary metabolite, 5-HIAA) in blood, plasma, urine, or cerebrospinal fluid (CSF), between people with depression and healthy controls.
Experiments artificially lower serotonin by depleting dietary tryptophan (its precursor). A 2007 meta-analysis and follow-up studies on hundreds of healthy volunteers found no induction of depressive symptoms.
Large-scale studies (e.g., one with 115,257 participants and another meta-analysis of 43,165) examined variations in the SERT gene and found no link to depression risk, even when factoring in stressful life events. Stress, trauma, inflammation, and brain circuit changes, strongly predicts depression, independent of serotonin genetics.
Moncrieff J, Cooper RE, et al. (2023). The serotonin theory of depression: a systematic umbrella review of the evidence. Molecular psychiatry, 28(8), 3243–3256. https://doi.org/10.1038/s41380-022-01661-0
Culverhouse RC, Saccone NL, et al. (2018). Collaborative meta-analysis finds no evidence of a strong interaction between stress and 5-HTTLPR genotype contributing to the development of depression. Molecular psychiatry, 23(1), 133–142. https://doi.org/10.1038/mp.2017.44
Leaving SSRIs could take 1-2 years, including Post-SSRI sexual dysfunction (PSSD), violence and suicide. Watch! Tucker Carlson.
Hijacked patients are kept in pharma-mental-prison with withdrawal threats, while hiding them the availability of clinical manuals with safe-tapering guidelines. Why isn’t the HHS publishing one like:
Horowitz M & Taylor DM. The Maudsley Deprescribing Guidelines: Antidepressants, Benzodiazepines, Gabapentinoids and Z-drugs. January 2024. Wiley-Blackwell. ISBN: 978-1-119-82302-5. (summary presentation, read this)
The same withdrawal problem happens with anti-epileptic drugs, hiding that some epilepsy is vax linked.
Ban any vaccines and drugs during pregnancy, unless a documented risk-benefit analysis, especially SSRIs and SNRIs: animal and human studies showed increased risk for miscarriage, low-weight / pre-term birth, hyperactive amygdala (“when they hit adolescence, their rates of depression go up, which is what we see in our mouse studies”) and congenital malformations. Humans, pulmonary hypertension, serious (84%) abstinence symptoms: jitteriness, poor muscle tone, weak cry, abnormal crying, respiratory distress, seizure, abnormal behavior, sleep abnormalities, poor feeding, vomiting, uncoordinated sucking and lethargy. A large dose-responsive study showed that counselling cut pre-term birth risk by 18%, while antidepressants increased it by 31 %.
Study the revolution of repurposed drugs for cancer: ivermectin, fenbendazole, etc.
Ban abortion drugs (n.b. misoprostol and mifepristone, recently FDA approved under your watch, as 2nd generic), not only because of the murdered babies, but of the life-risk for the mothers. Until they are banned, at least:
Mandate that the abortion reversal pills be sent together with the abortion ones, informing about the critical window for abortion reversal after taking the abortion pills.
Ban mailing of abortion drugs.
Require informed consent on the risks, and about the baby’s uninterrupted development since conception, and help available to vulnerable mothers.
Require all abortuaries to have emergency resources for botched abortions: even pro-abortionists agree that abortion should only involve murdering the unborn, not the mothers.
Make all those, directly or indirectly, involved in an abortion liable to damages including botched abortions, PTSD (Post-Traumatic Stress Disorder), PASS (Post-Abortion Stress Syndrome), infertility, miscarriages of future wanted babies, disabilities of future wanted babies, etc.
Mandate pro-life messages in pregnancy test package inserts, including the baby’s uninterrupted development since conception, and help available to vulnerable mothers.
Study the impact of agrichemicals in alergies (especially Celiac disease) and chronic diseases. Maybe it’s not so much the ultra-processing of food, but of poison in the food ingredients! Why are there no HHS studies comparing real organic-fed children with poison fed?
Note for readers: change to organic food definitions involves loopholes that have allowed industrial practices under the USDA Organic label, leading to consumer confusion and the creation of alternative certifications like the farmer-led Real Organic Project and Regenerative Organic Certification.
Study the impact of infant formula, comparing breast-babies with formula-babies in the long run. “Formula-fed babies are sicker, sick more often, and are more likely to die in infancy or childhood. ... In a recent case-control study, children with autism were found to be significantly more likely to have been formula-fed rather than breastfed” (this could be because working mothers tend to vax more their children but we need to rule out the formula).
Promote breast milk and milk banks!
Promote herbal medicine at the CDC and FDA pages! Research herbal medicine from all peoples: Chinese, Hindu, African, Native American, etc. Make a manual for each ailment and disease.
Study if mammographies cause breast cancer!
Study the impact of EMFs (ElectroMagnetic Frequencies) on health, then ban 5G and 4G MIMO, recommend WICAP instead of cellphone macro-towers, and reduce maximum radiation to Switzerland levels (100x lower limit!).
1 image = 1k words
Imagine your brain when you place your phone near it!

And there are many other ideas that I could add, or that people could add in the comments section of this article.
We appreciate all your efforts. Lives are at stake!
We’ll keep praying for you and your team!
Press release from the HHS
22 Sep 2025: “Following the label update for ASD, state Medicaid programs will be able to cover leucovorin for the indication of ASD, in partnership with the Centers for Medicare & Medicaid Services (CMS).
Note: don’t confuse with folinic with folic acid. Thought both are forms of vitamin B9, essential for cell growth and development, they differ in their chemical structure and metabolic function.
NIH will launch confirmatory trials and new research into the impact of leucovorin including safety studies (are you kidding? it’s vitamin B9!)
While promising, it is important to note that leucovorin is not a cure for ASD and may only lead to improvements in speech-related deficits for a subset of children with ASD.”
NIH recipients of the Autism Data Science Initiative (ADSI), were 13 projects totaling more than $50 million to transform autism research. ADSI integrates large-scale biological, clinical, and behavioral data with an exposomics approach that examines environmental, nutritional, medical, and social factors alongside genetics.
This is the study against Tylenol cited by the HHS:
“Cord biomarkers of fetal exposure to acetaminophen were associated with significantly increased risk of childhood ADHD and ASD in a dose-response fashion. Our findings support previous studies regarding the association between prenatal and perinatal acetaminophen exposure and childhood neurodevelopmental risk …”
Ji, Y., Azuine, R. E., Zhang, Y., Hou, W., Hong, X., Wang, G., Riley, A., Pearson, C., Zuckerman, B., & Wang, X. (2020). Association of Cord Plasma Biomarkers of In Utero Acetaminophen Exposure With Risk of Attention-Deficit/Hyperactivity Disorder and Autism Spectrum Disorder in Childhood. JAMA psychiatry, 77(2), 180–189. https://doi.org/10.1001/jamapsychiatry.2019.3259
Paracetamol-Autism Studies
Prada, Diddier, et al. “Evaluation of the Evidence on Acetaminophen Use and Neurodevelopmental Disorders Using the Navigation Guide Methodology.” Environmental Health 24, Article no. 56 (2025). https://ehjournal.biomedcentral.com/articles/10.1186/s12940-025-01208-0
Kristensen, David Møbjerg, et al. “Prolonged exposure to acetaminophen during pregnancy reduces testosterone production by the human fetal testis.” Science Translational Medicine 9, no. 388 (2017). https://pmc.ncbi.nlm.nih.gov/articles/PMC5451610/
Bauer, A. Z., Swan, S. H., Kriebel, D., Liew, Z., Taylor, H. S., Bornehag, C. G., Andrade, A. M., Olsen, J., Jensen, R. H., Mitchell, R. T., Skakkebaek, N. E., Jégou, B., & Kristensen, D. M. (2021). Paracetamol use during pregnancy - a call for precautionary action. Nature reviews. Endocrinology, 17(12), 757–766. https://doi.org/10.1038/s41574-021-00553-7
Cáceres, Marco. “Acetaminophen Linked to Autism and Other Neurological Disorders in Children.” The Vaccine Reaction, October 6, 2022. Reposted on GreenMedInfo. www.greenmedinfo.com/blog/tylenol-damages-brains-children-research-reveals
Parker, William, Ph.D. “Tylenol Damages The Brains of Children, Research Reveals.” GreenMedInfo, December 22, 2018. www.greenmedinfo.com/blog/tylenol-damages-brains-children-research-reveals
Lau, Jay. “Using Acetaminophen During Pregnancy May Increase Children’s Autism and ADHD Risk.” Harvard T.H. Chan School of Public Health News, August 20, 2025. https://hsph.harvard.edu/news/using-acetaminophen-during-pregnancy-may-increase-childrens-autism-and-adhd-risk/
There are dozens more!
Lawsuit
From a mother of autistic child, for no-warning label about paracetamol during pregnancy, dismissed in 2023 NY court because of failure to prove cause:
https://nysd.uscourts.gov/sites/default/files/pdf/MDL/22mc3043/Opinion%203.pdf
ASD-Tylenol: low correlation
Tylenol (acetaminophen/paracetamol) was first marketed as a prescription drug in the US. Also, it was first made available for as Tylenol Elixir for Children.
Johnson & Johnson bought the company and lobbied Government.
It became available over-the-counter.
Evidence showed that aspirin affected blood platelets and increased the risk of fetal harm in the third trimester: acetaminophen became the preferred and default pain reliever for pregnant women.
US Surgeon General issued public advice against giving aspirin to children with influenza or chickenpox, linking it to Reye’s syndrome, which can lead to brain swelling and liver damage.
FDA advised pregnant women to avoid nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen (Advil) and naproxen (Aleve) after 20 weeks of gestation due to the risk of fetal kidney problems: acetaminophen became the safest option.
If paracetamol in pregnancy was the primary cause of autism, we’d observe several effects that didn’t happen:
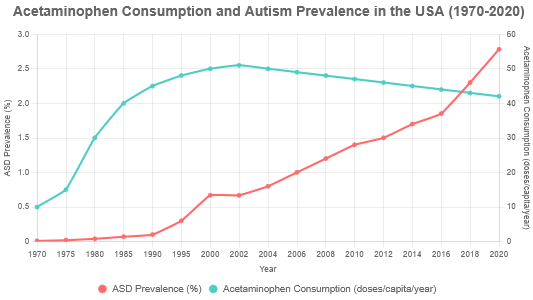
3 inflection points: 1970, 1982 and 2020
an exponential consumption of paracetamol to match the exponential autism
For example, if we use Bobby’s common sense rule, those born before 1970, should have received less maternal paracetamol than the younger born after 1970, but there’s little difference in the early autism rate.
ChatGPT.com and Claude.ai failed to chart acetaminophen consumption against autism rate. Unless hallucinating, Grok.com shows that there’s no correlation after 2002, when per capita Tylenol consumption went down:
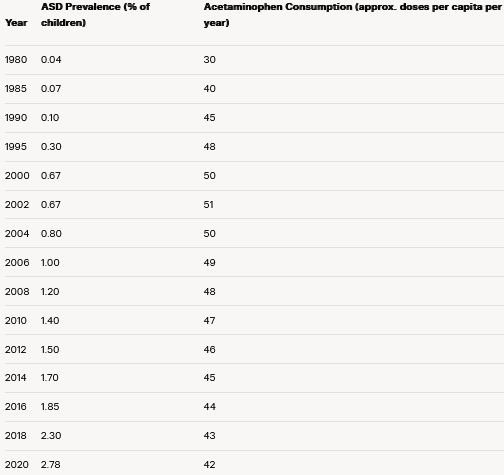
Data Sources and Methodology
Acetaminophen Consumption:
Pre-1980 data is estimated from historical market trends. Acetaminophen use was low in the 1970s (Tylenol gained U.S. market approval in 1955 but was niche until aspirin’s link to Reye’s syndrome in the late 1970s/early 1980s spurred growth).
Post-1980, consumption rose sharply, peaking around 2000, then stabilized or slightly declined based on prescription data (6 million in 2004 to 5.3 million in 2021) and OTC usage surveys (~23% of adults, ~52 million weekly users).
Approximations are in doses per capita per year, scaled from prescription volumes (assuming 500 mg/dose, ~10-20% of total use) and OTC market reports. Sources include:
Statista/ClinCalc: https://www.statista.com/statistics/781739/acetaminophen-prescriptions-number-in-the-us/
PMC (Slone Survey, 2006): https://www.bu.edu/slone/files/2012/11/SloneSurveyReport2006.pdf
PMC (Trends, 2011-2016): https://pmc.ncbi.nlm.nih.gov/articles/PMC6475729/
Autism Prevalence:
Pre-2000 data is based on retrospective studies and older diagnostic criteria (e.g., DSM-II in 1970s, DSM-III in 1980). Prevalence was ~0.01–0.04% in the 1970s, rising to ~0.1% by 1990 due to diagnostic shifts (e.g., DSM-III-R in 1987).
Post-2000, CDC’s ADDM Network provides reliable data: 1 in 150 (0.67%) in 2000 to 1 in 36 (2.78%) in 2020. The rise reflects broader diagnostic criteria (DSM-IV in 1994, DSM-5 in 2013), increased screening, and awareness, though environmental factors are debated.
Sources: CDC ADDM reports, historical studies via PMC (e.g., https://pmc.ncbi.nlm.nih.gov/articles/PMC3513384/).
ASD-maternal Tylenol: low correlation
Similar as above, there’s no correlation after 2010 between autism rate and maternal consumption of paracetamol:
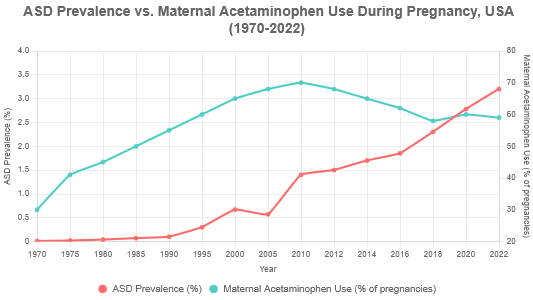
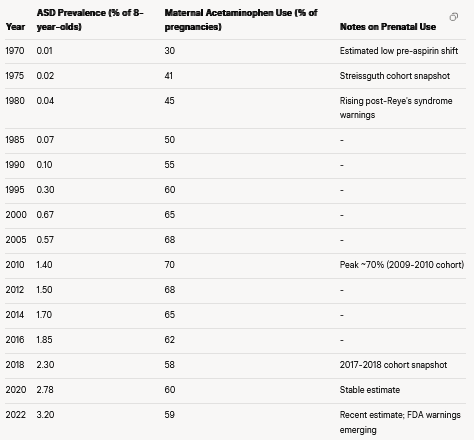
Maternal Acetaminophen Use During Pregnancy: Acetaminophen is the most common OTC pain/fever reliever in pregnancy (>50-65% usage). Historical trends are limited (OTC data isn’t systematically tracked like prescriptions), but available cohort studies show a rise from the 1970s (post-aspirin warnings) to the 2000s, followed by stabilization or slight decline amid safety concerns. Key snapshots:
1974-1975: ~41% use in first half of pregnancy (Streissguth et al., 1987 cohort).
2004-2018: Overall 62%, peaking at ~70% (2009-2010) and declining to 58% (2017-2018) per Generation R Next and other U.S. cohorts.
General estimates: 40-65% across studies; ~20% use >20 days.
Association: Meta-analyses (e.g., Masarwa et al., 2018; Ricci et al., 2023) report a modest increased ASD risk (pooled OR ~1.19, 19% higher odds) with prenatal exposure, especially longer duration or second/third trimester. However, evidence is mixed—some large studies (e.g., 2024 JAMA sibling analysis) find no causal link after controlling for confounders. Recent FDA action (Sept 2025) initiates label updates warning of potential risks, balancing benefits for maternal health.
Both trends show increases from the 1970s-2000s, but ASD rises more steeply post-2000 while prenatal use plateaus/declines slightly.
Tylenol = escape goat
At the press conference, Kennedy recognized that acetaminophen doesn’t explain all Autism.
Yet, they showcased Tylenol, avoiding a serious discussion about haccines.
Tylenol = smokescreen
The pathways of how Paracetamol causes autism were explained, yet Tylenol is at most, small proportion of autism agents.
It’s common sense: paracetamol sales haven’t followed the horrific exponential rise of autism.
https://www.cdc.gov/autism/data-research/
https://www.cdc.gov/autism/data-research/data-table.html
Just as the removal of mercury from vaccines, the banning of Tylenol from pregnancy will not have a measurable effect in stopping the rise in the autism rate, because the root cause is unrelated.
How do we know that? common sense: autism grew exponentially while paracetamol consumption didn’t, which means there’s an exponential driver.
Counting with thousands of studies pointing to vaccines as the main driver behind the exponential pandemic of autism, why isn’t it possible a meta-analysis, previously removing all studies funded or done by those involved in the COVID psy-op?
Key objection: vaccine uptake hasn’t increased exponentially, right?
To answer that, I used Grok AI, because I couldn’t find that analysis anywhere in the internet, which means that this might be an original discovery:
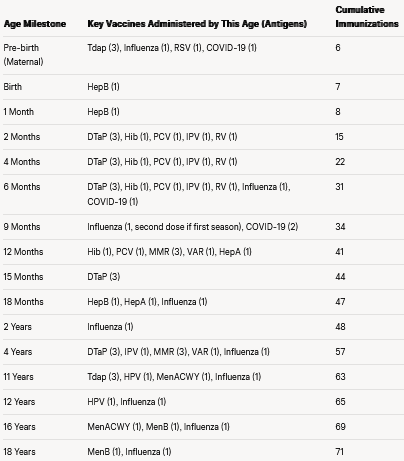
Cumulative immunizations
One injection could imply several immunizations, e.g. MMR counts as 3 immunizations (one for Measles, 1 for Mumps and 1 for Rubella).
Let’s analyze cumulative immunizations by age and along years.
Chart: Cumulative Immunizations by Age
Cumulative immunizations by age 18
US Schedule, incl. pre-born/maternal
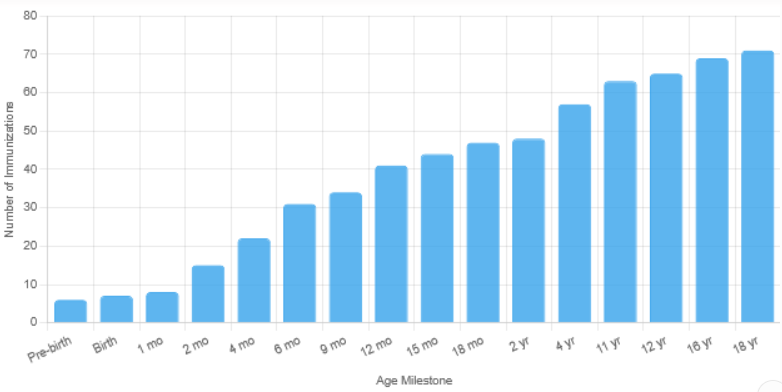
Notes:
Pre-birth assumes all recommended/optional maternal vaccines: Tdap (27–36 weeks), influenza (any trimester if season), RSV (32–36 weeks, Sept–Jan), COVID-19 (shared decision).
Influenza: 2 doses in first season (6 and ~7–9 months), then 1 annually (counted at milestones: 6mo, 9mo, 18mo, 2y, 4y, 11y, 12y, 16y, 18y for simplicity; actual adds more annually).
COVID-19: 3-dose series (6mo, ~7–8mo, ~9mo); no routine boosters counted beyond initial.
RSV: Maternal vaccine replaces infant mAb; if no maternal RSV, add infant mAb (1) at birth/6mo instead.
Actual injections fewer due to combinations (e.g., Pediarix = DTaP + HepB + IPV).
Milestones match the original graph; added 9 months for initial flu/COVID series completion.
Has the CDC ever studied the full 72-dose vaccine schedule given to children?
“NO”
This is the basis of a federal lawsuit demanding that the agency finally studies them.
Lead attorney Rick Jaffe, Esq., represents 2 physician plaintiffs, Dr. Paul Thomas and Dr. Ken Stoller, who argue that the CDC has failed in its legal and scientific duty to ensure the safety of its own recommended schedule.
Cumulative immunizations by age 80
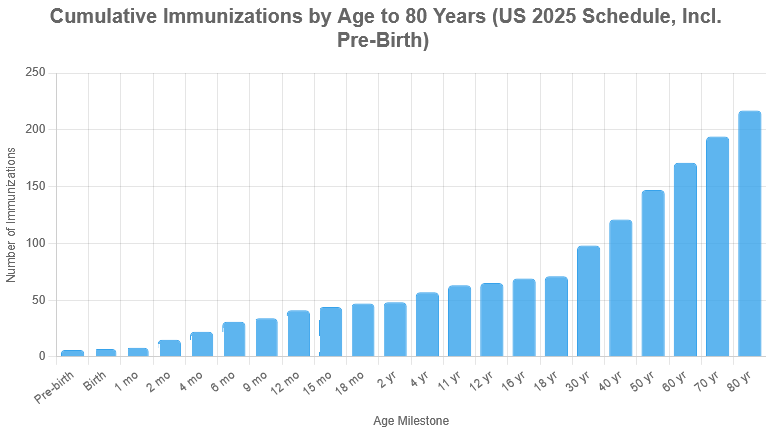
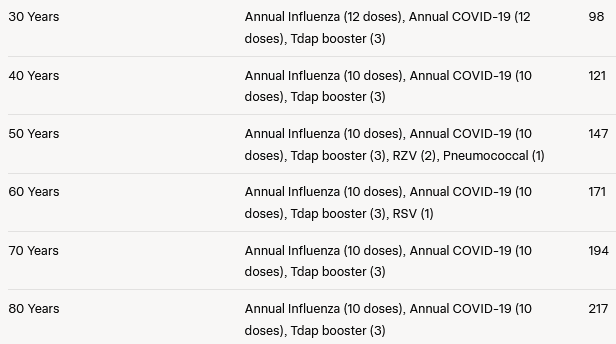
Notes:
Adult increments: Calculated for periods between milestones (e.g., 19-30 years = 12 years of annual flu/COVID + 1 Tdap booster at 21).
Tdap boosters: At ~21, 31, 41, 51, 61, 71 years.
Shingles (RZV): 2 doses at 50; Pneumococcal: 1 dose at 50 (2025 update).
RSV: 1 dose at 60 (shared decision).
Actual doses may vary; annual flu/COVID add ~2 per year post-18. Combinations reduce injections, but antigens counted separately.
Conclusion
The charts are impressive. In 1960, with 12 immunizations, everybody was happy, there were no terror deadly plagues and there was no autism.
Do we really need 71 immunizations for minors (ca. 6x, 600% more)?
Do we really need 217 lifetime immunizations?
Why was HepB vax forced into the schedule for newborns when it’s an STI?
Isn’t it unreasonable not to conclude that the inflated mandates are tied to Government capture by the Pharmafia?
Cumulative Immunizations Up to 3 Years
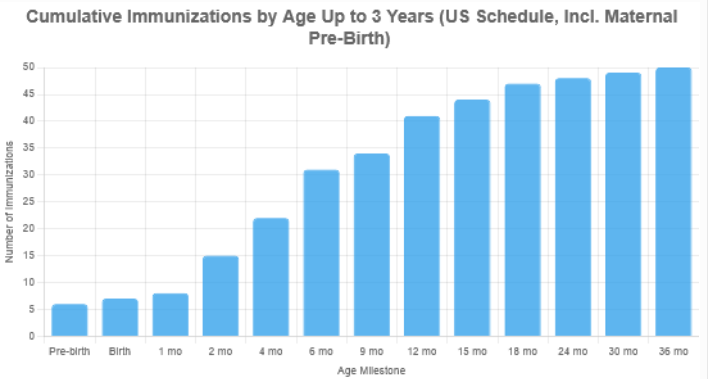
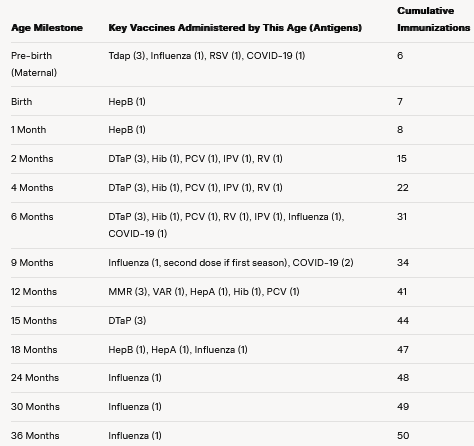
Notes:
2025 CDC recommended child and adolescent immunization schedule: cumulative number of individual immunizations (antigens) up to age 3 years to include maternal vaccinations during pregnancy as a “Pre-birth” category. These provide passive immunity to the newborn and are counted separately (e.g., Tdap = 3 for diphtheria, tetanus, pertussis; single-antigen vaccines like influenza, RSV, and COVID-19 = 1 each).
Pre-birth: Tdap (weeks 27-36), influenza (any trimester, if flu season), RSV (weeks 32-36, Sept-Jan), COVID-19 (optional, included as requested).
Influenza: Maternal dose + child’s own (2 doses in first season at 6 and ~7-9 months, then 1 annually at 18, 24, 30-36 months).
COVID-19: Maternal dose (optional); child series (optional for healthy kids, included): 3 doses (6, ~7-8, ~9 months).
RSV: Maternal vaccine precludes infant RSV mAb; if no maternal RSV, infant mAb (1) at birth would replace maternal RSV (1).
Actual injections may be fewer due to combination vaccines (e.g., Pediarix = DTaP + HepB + IPV in one shot, but antigens counted separately).
Cumulative Immunizations from conception to age 3 time series
US Schedule (1950–2025)
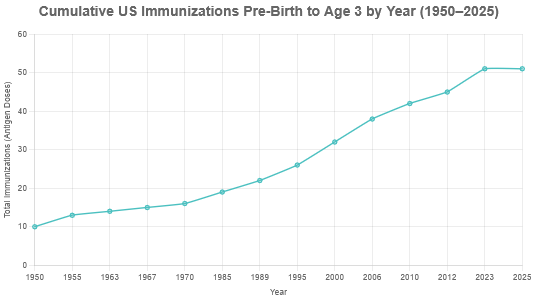

Notes:
Pre-2010, maternal vaccines limited to influenza (routine from 2004, counted from 2010 for child impact). Tdap maternal from 2012 (one-time in 2011, routine thereafter). RSV maternal 2023 (Abrysvo). COVID 2023 (optional/shared decision, included as routine).
Child counts include all doses up to 36 months; annual flu adds incrementally post-6 months.
Actual shots fewer via combinations (e.g., Pentacel = DTaP + IPV + Hib).
By 2025, protects against 18+ diseases; totals approximate based on standard series.
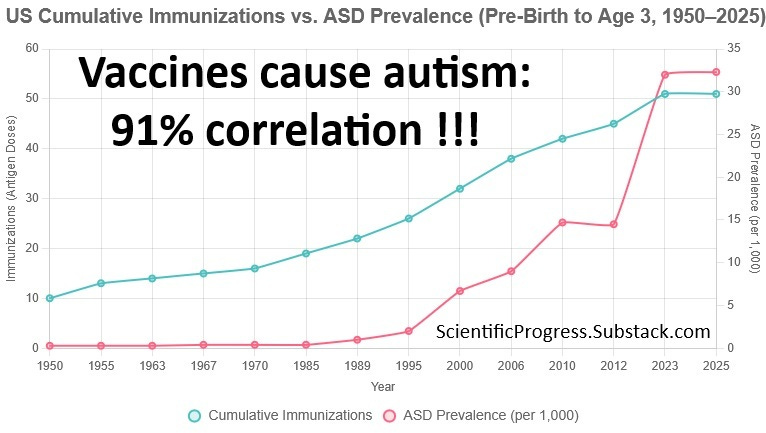
Cumulative Immunizations and ASD Prevalence Over Time
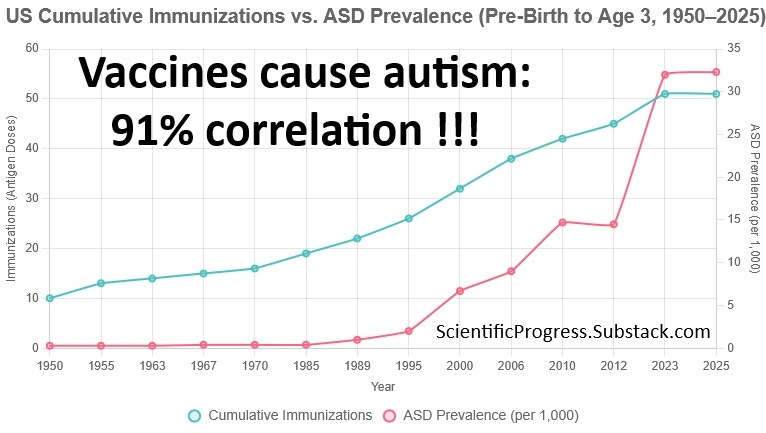
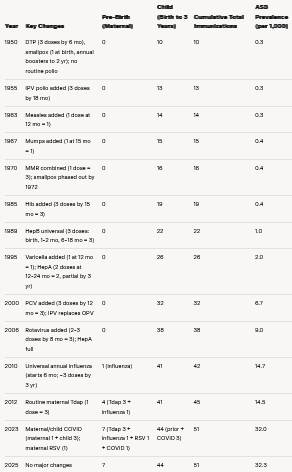
Note: ASD rates compiled from CDC ADDM (2000+), retrospective studies (pre-2000: e.g., ~0.3–0.4/1,000 in 1950–1985 from narrow criteria; rise post-1987 DSM-III-R broadening). 2025 uses 1:31 cited from the CDC by Kennedy at the 22 Sep 2025 conference.
DSM changes in ASD definition: bad excuse
The definition of autism spectrum disorder (ASD) has evolved significantly since the 1950s, driven by updates to the Diagnostic and Statistical Manual of Mental Disorders (DSM), published by the American Psychiatric Association (APA). Below is a concise timeline of key DSM changes in the definition and diagnostic criteria for autism and related disorders, focusing on their impact on ASD classification and prevalence. Pre-DSM-III (1980), autism was not formally defined in the DSM, so earlier descriptions draw from historical psychiatric literature and precursor terms.
Pre-DSM (1950–1952): No Formal ASD Category
Context: The term “autism” was introduced by Leo Kanner in 1943 to describe children with social withdrawal, communication deficits, and repetitive behaviors. It was considered a rare, severe condition, often linked to schizophrenia or “childhood psychosis.”
DSM-I (1952): No specific autism category. Children with autistic-like symptoms were classified under “Schizophrenic Reaction, Childhood Type” (code 000-x28), emphasizing psychotic features. Diagnosis was rare, with prevalence estimated at ~0.3–0.4 per 1,000, based on retrospective studies.
Impact: Narrow focus on severe cases; limited recognition of milder presentations.
DSM-II (1968): Continued Lack of Autism Category
Definition: Autism was still not a distinct diagnosis. The manual included “Schizophrenia, Childhood Type” (code 295.8), which vaguely encompassed symptoms like social withdrawal and developmental delays, sometimes applied to autistic children.
Change: Minimal; autism remained conflated with psychosis. Diagnostic criteria were vague, relying on clinician judgment.
Impact: Prevalence remained low (~0.4/1,000), as only extreme cases were identified, often misdiagnosed as schizophrenia or mental retardation.
DSM-III (1980): Introduction of Autism as a Distinct Disorder, no change in ASD rate trend
Definition: First inclusion of “Infantile Autism” under Pervasive Developmental Disorders (PDD), separating it from schizophrenia. Criteria required:
Onset before 30 months.
Pervasive lack of responsiveness to others.
Gross deficits in language development.
Peculiar speech patterns (e.g., echolalia), if speech present.
Bizarre responses to environment (e.g., resistance to change, attachments to objects).
Absence of delusions/hallucinations (ruling out psychosis).
Change: Formal recognition of autism as a developmental disorder, not psychosis. Introduced strict criteria, limiting diagnosis to severe, early-onset cases.
Impact: Prevalence slightly increased (~0.4–1/1,000) due to clearer diagnostic boundaries, but still restrictive. Excluded milder or later-onset cases.
DSM-III-R (1987): Broadened Criteria and New Subcategories
Definition: Renamed “Autistic Disorder” and placed under PDD. Criteria expanded to include:
Qualitative impairment in social interaction (e.g., lack of social/emotional reciprocity).
Communication deficits (e.g., delayed or absent language, impaired conversational skills).
Restricted, repetitive behaviors or interests (e.g., stereotypies, rituals).
Onset in infancy or childhood (less rigid age cutoff).
Added “Pervasive Developmental Disorder Not Otherwise Specified” (PDD-NOS) for subthreshold or atypical cases.
Change: Broader, more flexible criteria; inclusion of PDD-NOS captured milder or atypical presentations. Removed strict “infantile” focus.
Impact: Prevalence rose to ~1–2/1,000, as PDD-NOS allowed diagnosis of less severe cases. Increased recognition of variability in symptoms.
DSM-IV (1994) and DSM-IV-TR (2000): Introduction of Asperger’s and Subtypes
Definition: Expanded PDD category to include five disorders:
Autistic Disorder (similar to DSM-III-R but refined).
Asperger’s Disorder (new): Social impairment and restricted behaviors without significant language or cognitive delays.
PDD-NOS (retained for atypical cases).
Rett’s Disorder (genetic condition with autistic features).
Childhood Disintegrative Disorder (CDD, rare regression after normal development).
Criteria for Autistic Disorder required impairments in three domains (social, communication, behavior), with at least six symptoms from a checklist, and onset before age 3.
Change: Added Asperger’s and other subtypes, formalizing a spectrum-like approach. Detailed symptom checklists improved diagnostic consistency.
Impact: Prevalence increased significantly (~6.7/1,000 by 2000), driven by Asperger’s and PDD-NOS diagnoses, which captured higher-functioning individuals and those with milder symptoms.
DSM-5 (2013): Consolidation into Autism Spectrum Disorder
Definition: Merged Autistic Disorder, Asperger’s, PDD-NOS, and CDD into a single “Autism Spectrum Disorder” (ASD) category. Rett’s Disorder was excluded (recognized as genetic). Criteria:
Persistent deficits in social communication/interaction (merged social and communication domains).
Restricted, repetitive behaviors, interests, or activities.
Symptoms present in early development (but may manifest later).
Severity levels (1–3) based on support needed.
Specifiers for co-occurring conditions (e.g., intellectual disability, language impairment).
Change: Unified spectrum approach eliminated subtypes, emphasizing a continuum of severity. Removed strict age-of-onset and specific symptom counts, allowing flexibility. Added sensory sensitivities as a criterion.
Impact: Prevalence jumped (14.5/1,000 in 2012 to ~27.8/1,000 by 2020), as broader criteria captured more individuals, especially those with milder symptoms or later diagnoses. Diagnostic substitution from other disorders (e.g., ADHD) increased.
DSM-5-TR (2022): Minor Refinements
Definition: Retained ASD as a single category with minor clarifications:
Emphasized that symptoms can be identified “currently or by history” to support diagnosis in older children/adults.
Clarified co-occurring conditions (e.g., distinguishing ASD from ADHD or anxiety).
Updated terminology for consistency (e.g., aligning with neurodiversity language).
Change: No major overhaul; focused on improving diagnostic clarity and flexibility for diverse presentations.
Impact: Prevalence continued to rise slightly (32.0–32.3/1,000 by 2022–2025), reflecting ongoing improvements in screening and awareness rather than criteria changes.
Summary of Impact on Prevalence
1950–1980: Narrow criteria (psychosis-linked or severe autism) kept prevalence low (~0.3–0.4/1,000).
1987 (DSM-III-R): Broader criteria and PDD-NOS increased prevalence to ~1–2/1,000.
1994 (DSM-IV): Asperger’s and subtypes boosted prevalence to ~6.7/1,000 by 2000.
2013 (DSM-5): Unified spectrum and flexible criteria drove prevalence to ~27.8–32.3/1,000 by 2020–2025, amplified by screening and awareness.
The 2012-2023 jump
The jump in autism spectrum disorder (ASD) prevalence from 14.5 per 1,000 in 2012 to 32.0 per 1,000 in 2023 (as shown in the table) is primarily driven by non-biological factors related to diagnosis and surveillance, not an actual increase in autism incidence. Below, I outline the key reasons for this observed increase, based on CDC data and peer-reviewed studies:
1. Expanded Diagnostic Criteria
The release of the DSM-5 in 2013 significantly broadened the diagnostic criteria for ASD. It merged previously separate diagnoses (e.g., autism, Asperger’s syndrome, pervasive developmental disorder-not otherwise specified) into a single ASD category. This captured more individuals, especially those with milder symptoms or higher-functioning presentations.
DSM-5 also introduced a dimensional approach, allowing for diagnosis based on a spectrum of social-communication deficits and restricted/repetitive behaviors, increasing inclusivity compared to DSM-IV used in 2012.
2. Improved Screening and Awareness
Public and professional awareness of ASD has grown, leading to earlier and more frequent screening. Tools like the Modified Checklist for Autism in Toddlers (M-CHAT) became widely used in pediatric settings by the 2010s, identifying more cases at younger ages.
Campaigns by organizations like Autism Speaks and CDC’s “Learn the Signs. Act Early.” program (expanded post-2010) encouraged parents and clinicians to recognize subtle signs, boosting diagnosis rates.
3. Better Access to Diagnostic Services
Between 2012 and 2023, access to developmental evaluations improved, particularly in underserved communities. CDC’s Autism and Developmental Disabilities Monitoring (ADDM) Network expanded its surveillance sites, capturing more diverse populations.
Policy changes, such as increased insurance coverage for developmental assessments (e.g., under the Affordable Care Act), facilitated more diagnoses.
4. Inclusion of Milder Cases
The 2020 and 2022 ADDM reports (informing 2023 data) noted a higher proportion of children diagnosed with ASD without intellectual disability (IQ > 70), reflecting a shift toward identifying milder cases. In 2012, about 31% of ASD cases had no intellectual disability; by 2020, this was ~52%.
This shift is partly due to diagnostic substitution: children previously labeled with other developmental or behavioral disorders (e.g., ADHD, learning disabilities) are now more likely to receive an ASD diagnosis.
5. Methodological Changes in Surveillance
The ADDM Network refined its methodology post-2012, improving case ascertainment. For example, the 2020 report (used for 2023 estimates) included more comprehensive record reviews (e.g., school and medical records) and adjusted for underdiagnosis in earlier years.
Changes in data collection, like including children with suspected ASD (not just confirmed diagnoses), contributed to higher prevalence estimates.
6. Societal and Cultural Factors
Increased societal acceptance of neurodiversity reduced stigma, encouraging families to seek diagnoses for access to services (e.g., IEPs, therapies). This is particularly evident in higher-income and urban areas, where prevalence rates are often higher due to resource availability.
Community-level variations in diagnostic practices also play a role, with some regions reporting higher rates due to proactive screening.
Quantitative Context
2012: ADDM reported 1 in 69 children (~14.5/1,000) based on 2010 data, using DSM-IV-TR criteria, with fewer milder cases identified.
2023: ADDM’s 2020 data (published 2023) reported 1 in 36 (~27.8/1,000), rising to ~32/1,000 in preliminary 2022 estimates. The 2025 estimate (32.3/1,000) aligns with this trend.
ASD: not a diagnosis epidemic
Kennedy explained that the rise of the autism rate isn’t due to a change in diagnostic-criteria, and that it can be proven with common sense, because people older than 50 don’t have deep autism (non-verbal, head banging, etc.) and there are dozens of studies proving it’s not only about better diagnostics tools for children.
Kennedy cited the UC Davis M.I.N.D. Institute, which has investigated the increase in autism diagnoses and found that it cannot be explained by changes in diagnosis and counting alone.
Here’s a quick glance:
Byrd, R. S., Sage, J., Keyzer, J., Stephens, B., Wiggins, L. D., Lee, L. C., ... & Schendel, D. E. (2002). Report to the legislature on the principal findings from the epidemiology of autism in California: A comprehensive pilot study. UC Davis M.I.N.D. Institute. https://www.sciencedaily.com/releases/2002/10/021018081039.htm
Hertz-Picciotto, I., Croen, L. A., Hansen, R., Jones, C. R., van de Water, J., & Pessah, I. N. (2006). The CHARGE study: An epidemiologic investigation of genetic and environmental factors contributing to autism. Environmental Health Perspectives, 114(7), 1119–1125. https://doi.org/10.1289/ehp.8483
King, M., & Bearman, P. S. (2009). Diagnostic change and the increased prevalence of autism. International Journal of Epidemiology, 38(5), 1224–1234. https://doi.org/10.1093/ije/dyp261
Hertz-Picciotto, I., & Delwiche, L. (2009). The rise in autism and the role of age at diagnosis. Epidemiology, 20(1), 84–90. https://doi.org/10.1097/EDE.0b013e3181902d15
Hertz-Picciotto, I., Schmidt, R. J., & Krakowiak, P. (2018). Understanding environmental contributions to autism: Causal concepts and the state of science. Autism research : official journal of the International Society for Autism Research, 11(4), 554–586. https://doi.org/10.1002/aur.1938
And there are hundreds more, for example:
Twin and Heritability Studies
Hallmayer, J., Cleveland, S., Torres, A., Phillips, J., Cohen, B., Torigoe, T., ... & Risch, N. (2011). Genetic heritability and shared environmental factors among twin pairs with autism. Archives of General Psychiatry, 68(11), 1095-1102. https://doi.org/10.1001/archgenpsychiatry.2011.76
Sandin, S., Lichtenstein, P., Kuja-Halkola, R., Hultman, C., Larsson, H., & Reichenberg, A. (2017). The heritability of autism spectrum disorder. JAMA, 318(12), 1182-1184. https://doi.org/10.1001/jama.2017.12141
DNA mutations after birth
(not inherited but environmental, mostly vax autism)
Deisher, T. A., Doan, N. V., Omaiye, A., Koyama, K., & Mann, S. (2014). Impact of environmental factors on the prevalence of autistic disorder after 1979. Journal of Public Health and Epidemiology, 6(9), 271-284. https://doi.org/10.5897/JPHE2014.0649
Sanders, S. J., Murtha, M. T., Gupta, A. R., Murdoch, J. D., Raubeson, M. J., Willsey, A. J., Ercan-Sencicek, A. G., DiLullo, N. M., Parikshak, N. N., Stein, J. L., Walker, M. F., Ober, G. T., Teran, N. A., Song, Y., El-Fishawy, P., Murtha, R. C., Choi, M., Overton, J. D., Bjornson, R. D., Carriero, N. J., … State, M. W. (2012). De novo mutations revealed by whole-exome sequencing are strongly associated with autism. Nature, 485(7397), 237–241. https://doi.org/10.1038/nature10945
O’Roak, B. J., Vives, L., Girirajan, S., Karakoc, E., Krumm, N., Coe, B. P., Levy, R., Ko, A., Lee, C., Smith, J. D., Turner, E. H., Stanaway, I. B., Vernot, B., Malig, M., Baker, C., Reilly, B., Akey, J. M., Borenstein, E., Rieder, M. J., Nickerson, D. A., … Eichler, E. E. (2012). Sporadic autism exomes reveal a highly interconnected protein network of de novo mutations. Nature, 485(7397), 246–250. https://doi.org/10.1038/nature10989
Wang, T., Guo, H., Xiong, B., Stessman, H. A., Wu, H., Coe, B. P., Turner, T. N., Liu, Y., Zhao, W., Hoekzema, K., Vives, L., Xia, L., Tang, M., Ou, J., Chen, B., Shen, Y., Xun, G., Long, M., Lin, J., Kronenberg, Z. N., … Eichler, E. E. (2016). De novo genic mutations among a Chinese autism spectrum disorder cohort. Nature communications, 7, 13316. https://doi.org/10.1038/ncomms13316
Environmental Factor Studies
Modabbernia, A., Velthorst, E., & Reichenberg, A. (2017). Environmental risk factors for autism: An evidence-based review of systematic reviews and meta-analyses. Molecular Autism, 8, 13. https://doi.org/10.1186/s13229-017-0121-4
Bölte, S., Girdler, S., & Marschik, P. B. (2019). The contribution of environmental exposure to the etiology of autism spectrum disorder. Cellular and molecular life sciences : CMLS, 76(7), 1275–1297. https://doi.org/10.1007/s00018-018-2988-4
Oommen, A., AlOmar, R. S., Osman, A. A., & Aljofi, H. E. (2018). Role of environmental factors in autism spectrum disorders in Saudi children aged 3-10 years in the Northern and Eastern regions of Saudi Arabia. Neurosciences (Riyadh, Saudi Arabia), 23(4), 286–291. https://doi.org/10.17712/nsj.2018.4.20180170
Gene-Environment Interaction Studies
Tordjman, S., Somogyi, E., Coulon, N., Kermarrec, S., Cohen, D., Bronsard, G., ... & Xavier, J. (2014). Gene × environment interactions in autism spectrum disorders: Role of epigenetic mechanisms. Frontiers in Psychiatry, 5, 53. https://doi.org/10.3389/fpsyt.2014.00053
Karimi, P., Kamali, E., Mousavi, S. M., & Karahmadi, M. (2017). Environmental factors influencing the risk of autism. Journal of Research in Medical Sciences, 22, 27. https://doi.org/10.4103/1735-1995.200272
Meta-Analyses on Environmental Risk Factors
Wan, H., Zhang, C., Li, H., Luan, S., & Liu, C. (2018). Association of maternal diabetes with autism spectrum disorders in offspring: A systematic review and meta-analysis. Medicine, 97(2), e9438. https://doi.org/10.1097/MD.0000000000009438
Rai, D., Lee, B. K., Dalman, C., Golding, J., Lewis, G., & Magnusson, C. (2013). Parental depression, maternal antidepressant use during pregnancy, and risk of autism spectrum disorders: Population based case-control study. BMJ, 346, f2059. https://doi.org/10.1136/bmj.f2059
Conclusion: near perfect correlation between immunizations and ASD !!!
The Pearson correlation coefficient between cumulative immunizations and ASD prevalence is 0.91 (strong positive linear association, p < 0.001), calculated as:
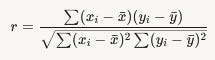
where x = immunizations, y = ASD rates.
Whether intended or not, changing the definition of autism over time resulted in data obfuscation.
The correlation coefficient should be higher than 0.91 if a consistent standard definition of severe autism is applied. Another way to solve the obfuscation is to use data from other countries which didn’t change the definition at all, or changed them in a different year than the USA.
It won’t reach perfect correlation (1) because several other “environmental” factors may have a smaller yet measurable impact on ASD and children brain injuring:
illegal drugs
opioids
medicines taken during pregnancy
agrichemically toxic and genotoxic food
industrial, agrichemical and pharmaceutical pollution in water
EMF
doppler sonograph/ultrasound
Etc.
That’s the job the HHS hasn’t been doing!
Not all correlation is causation,
but stronger correlation
demands stronger explanation
to refute probable relation.
Why didn’t HHS Secretary Kennedy present all this in the press conference?
9 steps out of global tyranny
Sep 10

Time after time, most have become disappointed with their political leaders, in whom they placed their hopes for change. What they don’t realize is that the root of the problem is the system:
The PLAN revealed

This research took many many hours (including late night work), that will save you that amount of reading and organizing ideas. If you like it, please consider a paid subscription:
Are you prepping?
They are manufacturing a the huge infrastructure and financial crisis !
Have food and water for 3 weeks !
Yellow alert: global cyber-storm
20 December 2024

Due to the urgency, I’m not including the usual footnotes supporting everything I write. I’m working on the promised pieces. In the meantime, I’ll be releasing some articles I had been baking for a while, which needed polishing.
20 laws we need to exit Extermination Planet
Laws to exit planet prison

No Free Speech without Reach

Why was Bill Gates the mentor of Zuckerberg?
Zuckerberg really flipping?
15 Jan

What Has Happened To Mark Zuckerberg?
How Rumsfeld forced the approval of lethal Aspartame.
Artificial sweeteners, MSG, PFAS, Glyphosate ... go organic!
Why is food poisoning legal?
26 November 2023

This article would be another tool you could share to keep waking-up the still-trusting sleepwalkers: some reject discussing injections, but they’d be open to food.
Solutions for "this" Democracy?

Rethinking science
19 December 2023

Unless we change it, we’re doomed to the next PLANdemic. And yet, nothing has changed, only got worse! This isn’t pessimism: just a realistic call to ACTION in the medical and scientific freedom communities.
Rethinking education for the real 21st century:
Why not earning $60,000 per year for educating your own children?

Call to action
1. Please share in social networks!
10 shares = waking up more people + especial gratitude:
Waking others up SAVES lives or livelihoods.
For example, send them free ebooks:
Vax-Unvax: Let the Science Speak
The more the awakened, the sooner this nightmare will be over !
2. Please subscribe
Scientific Progress is a reader-supported publication. To receive new posts and support my work, please consider becoming a free or paid subs:
3. Show your love in the tip jar =)
1 dollar makes a difference !

4. Please consider “buy me a coffee”:

5. Please reconsider a paid subscription:
6. Please consider commissioning an article for the topic of your preference:
7. Pray
Most important of all: let’s pray for each other and the conversion of our enemies !
The evil we see in the material world is just the echo from the spiritual battle between God and Satan and their followers, either human or angelic.
Darkness grows because the light of faith is fading. Faith is the root of a plant that withers without the sunlight of love and the water of prayer. God is love: ask Him for more faith in love.
Nothing. Its all distraction. Bread & circuses to entertain the masses.
Just like Trump saying he wants the killing to stop and yet keeps selling arms to Israel & Ukraine.
I pray 🙏🏼 this letter gets shared over and over again. It’s disappointing at the very least to see the vice grip Big Pharma cartels have kept American politicians trapped in… it’s a crime how many people Big Pharma has killed, maimed, harmed and left dependent on sick care for life… it’s discouraging to realize how many Americans have been hypnotized into believing their doctors know what’s best for them… but the biggest problem are the media drug pushers who will print or broadcast anything for the love of advertising money…